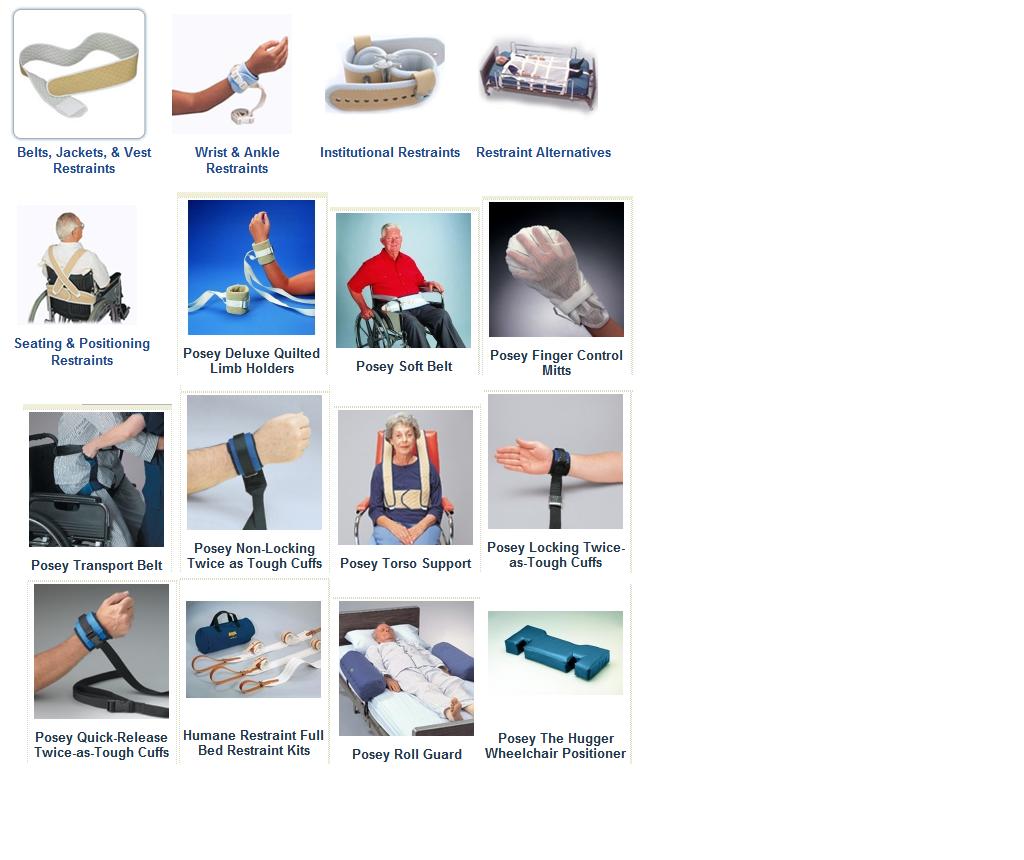
Patient Restraints:
CLEARLY, ALL INFORMATION PROVIDE HEREIN IS FOR REFERENCE ONLY!
All provided information supports the fact that Federal, State Laws must be followed without exception of fact. All facility policy and procedures must be followed. In the event of exception to fact, contact your direct NurseLine Healthcare Supervisor and the facility supervisor for direction.
Types of Restraints:
What Should I Know About Medical Restraints?
The FDA reported, in 1992, that over half a million patients in health care facilities need hospital restraints. Because of the increasingly aging population, it's likely that number has increased. Medical restraints are generally used to prevent falls and, less commonly, to address behavioral problems.
Restraints are generally made of a durable material such as nylon or leather. The majority of the restraints are machine washable. In the case of the leather medical restraints, sterilization can be achieved through the use of at least 70% isopropyl (rubbing) alcohol. Methods of sterilization such as autoclaving, steam and BTO gas are not recommended.What Kind of Restrictions are there on Selling Medical Restraints?
Federal law requires that anyone purchasing <B>Medical Restraints</B> must either be a physician, a medical facility, or have an order from a physician. In order to process your order, Vitality Medical must receive a copy of the prescription. Prescriptions may be faxed to 801-733-5797. Orders will not be shipped without a prescription. Before purchasing, see Vitality Medical's Return Policy.How Do I Know What Type of Restraint to Get?
Your physician or the treating physician will know what type of restraint to get. Accordingly to Findarticles.com, the Joint Commission on Accreditation of Healthcare Organizations(JCAHO) classifies restraints into three categories:
Class I Class II Class III
Wrist restraints only Roll belt only Geriatric wheelchair with table top Mitts Full bed rails Any combination of geriatric wheelchair, wrist restraint, and roll belt Vest restraint Restraints, opposite limbs Locked restraint, including leather Locked seclusion Enclosed bed Restraints, 4 limbs with or without roll belt Body net
You may want to ask some questions of the treating physician, such as: What type of medical restraint is needed (hand, ankle, seating, etc.)What type of material should the medical restraint be made out of (leather, nylon, etc.)?Does it need a lock? Not all restraints come with a lock.
You may also need to take a patient's measurement to ensure an accurate fit. When measuring, make sure not to hold the measuring tape too tight or too loose around the patient. Most medical restraints are adjustable, so a reasonably accurate measurement should be sufficient to purchase the correct medical restraint.Does My Insurance/Medicare/Medicaid Reimburse for Medical Restraints?
Insurance/medicare/medicaid reimbursement varies. Contact your insurance representative before purchasing medical restraints. Be aware that some insurance companies or institutions periodically review medical restraint reimbursement claims to ensure the medical restraints are being used properly. Vitality Medical does not bill insurance/medicare/medicaid for medical restraints or any other product.
What are Restraint Alternatives?
<B>Restraint Alternatives</B> are products that aren't traditional medical restraints. Currently, Vitality Medical sells two kinds of restraint alternatives: the <B>Posey Restraint Net</B> and the <B>Posey Roll Guard</B>.
The Posey Restraint Net is used for patients who pose extreme harm to themselves. The restraint net fits comfortably across the body and securely fixes the patient's arms and legs. The next is made of nylon and is machine washable.
The Posey Roll Guard is designed for patients who fall out of bed, but do not need restraints. Each Roll Guard acts as a cushion obstacle to prevent falling. The Roll Guards can also be placed in various places on the bed to relieve pressure on the patient. Each Roll Guard is has a machine-washable nylon and the vinyl inner pillows can be washed with liquid detergent.
Another alternative restraint worth considering is the Posey Roll Belt. This belt goes around the torso to protect the patient from rolling out of bed and falling to the floor. The Posey Roll Belt comes in various sizes to fit the needs of the individual patient.Below are two videos about preventing falls without restraints and some restraint options to help protect patients from injury.

In hospitals and nursing homes, it's sometimes necessary to restrain patients for safety reasons--usually to prevent them from harming themselves, but on occasion to keep them from hurting others. For example, restraints are used when a confused patient has pulled IVs or tubes out of his or her body. A wheelchair restraint may be used for someone who is likely to wander away and get lost.
IMPORTANT TIPS FOR THE USE OF PATIENT RESTRAINTS:
Physical patient restraints can be useful in protecting the patients/residents from falls and from wandering or straying. However, restraints are not the only solution to these difficulties and in some cases may be more dangerous. The following are important tips that can make more aware of when and how restraints should be used. It will also help you identify problems which could have serious consequences if not responded to.
Patient Rights:
Patients/residents have the right to be free from restraints. Restraint use should not be a first choice solution. Before allowing yourself or a loved one to be restrained, be sure to understand the reason for the restraint use, request a limited time frame for restraint use, and be sure that all other solutions to the problem have been exhausted.
Facility Policy:
All health care facilities must have a written policy on use of patient restraints. Ask to see this document and be sure that you understand and are comfortable with the policy set forth by your facility.
Prescription Device:
Restraints are prescription devices and may only be used if a physician, or other healthcare professional licensed to prescribe in your State, has specifically ordered a restraint for an individual. The need for the restraint must be well document in the patient chart and assessment of the need should continue even after the device has been ordered.
Patient Criteria:
Not all patients/residents are appropriate for restraint use. For example, an agitated or seriously confused patient may not be a good candidate for restraints. The use of restraints may only add to this agitation or confusion and place the patient in jeopardy as he/she may try to escape from the
device. These medical symptoms combined with the use of a restraint may lead to a serious injury or death.
Appropriate Size:
It is very important to be sure that the appropriate size o restraint is selected. A restraint that is too small will be uncomfortable for the patient and may cause agitation or constriction of bodily parts. A restraint that is too large or loose, where the patient can slide down or forward, may result in asphyxiation.
Good Labeling:
Manufacturers of patient restraints are being required to develop better labeling. They are also being encouraged to use graphic in improved labels, sewn directly on the device, to help ensure proper application. Look for these labels and alert a healthcare provider if it appears a device is on incorrectly or a patient is uncomfortable in a restraint.
Proper Use:
For wheelchair use, be sure that the patient is upright and securely seated in the chair before applying the restraint. See device directions for correct application. Incorrect applications is more likely to result in the patient sliding forward which may result in asphyxiation. For use in a bed, be sure the restraint is NEVER tied to the bed rails or mattress. The restraint should only be tied to the bed springs. Also, most restraint are not indicated for use with regular beds or regular chairs, including geri-chairs. Consult the manufacturer labeling for correct application of the restraint to any bed or chair.
Length of Wear:
Any patient/resident in a restraint must be free of that restraint at frequent intervals to ensure good patient health. Long-term immobilization can contribute to various health problems including decubitus ulcers, nerve damage, incontinence, and sensory deprivation. Consult with the facility policy for the maximum length of each period of restraint use. During the time when the patient is free of restraint, be sure that exercise, such as walking, is available and encouraged.
Patient Monitoring:
Patients/residents must be monitored frequently while wearing a restraint device. As with any other medical device, supervision and monitoring are critical to ensure the safety of the patient.
Question Facility Management for Policy and Procedures:
Ask your facility what alternatives exist or are being developed to reduce the use of restraints. Restraints should never be used a substitute for nursing care. They are an adjunct to proper care. In many cases, volunteers may be all a facility needs to help keep patients free from restraints. However, if you are aware of potential dangers of restraint use and know what to look for and what to do if you see a restraint being used incorrectly, it could save a patient from a serious injury or even death.
Instructions to be applied to patient as cited by Laws and in support of Facility requirements :
1 Determine that there is a valid need to restrain the patient. Consider your legal and ethical obligations as a health care worker, and realize that an individual shouldn't have his or her movement restricted simply for the caregiver's convenience.
2 Contact the patient's physician, and get an order for the use of restraints.
3 Decide which type of restraint is most appropriate for the situation. Use the least-restrictive device you can. Choose a belt or vest for patients who need to remain in a wheelchair, wrist or ankle restraints to restrict movement of hands or legs and mitten restraints for patients who scratch themselves or continually get out of wrist restraints.
4 Read the directions on the tag attached to the restraint, as each manufacturer and type of device has certain specifications. Pay attention to safety warnings, especially when using a vest, because the patient may suffocate if it's applied incorrectly. Ask a coworker for help if you're not sure how to use a restraint.
5 Apply the restraint correctly. Use a quick-release knot, also called a slipknot, to fasten devices that don't have a buckle. Fasten the ties to a part of the wheelchair that the patient can't easily get to. Place a call light within the patient's reach and make sure he or she knows it's there.
6 Check on restrained patients at least every 15 minutes. Remove the restraint at least every two hours to check for skin irritation and proper blood circulation, exercise the joints that are inhibited by the restraint and determine whether the device is still necessary.
7 Get a new order from a physician if the patient needs to be restrained the following day. By law, a doctor's order for restraints expires after 24 hours.
=================================================================
Tips & Warnings:
1.Ties must be fastened to a movable part of the frame if the wheelchair has an adjustable seat.
2.Make sure that the restraint isn't too tight, because it could interfere with blood circulation or breathing. However, the patient may be able to get out of the device if it's too loose.
3.Don't put a restraint in a location that could cause medical complications, such as over an incision or hernia.
1) Avoid it if at all possible. Use your powers of persuasion. Verbal judo speaks to several techniques that all public safety personnel can use to calm patients and convince them to cooperate.
Remember that much of your communication to the patient involves body language — standing over patients, crossing your arms over your chest, planting your feet in an aggressive position; any of these postures can interpreted as a threat by an already agitated patient.
2) Safety is paramount. Don't try to restrain the patient if you are not confident of the outcome. Even the smallest patient can put up a hella fight when provoked. If there are objects around that can be used as weapons, clear them out if you can. If there are weapons — well, I'd leave.
3) Plan your attack. Recognize that you will be "attacking" your patient. That action verb will remind you that you may be causing harm. Plan accordingly to minimize injury. While one person engages conversation with the patient, others should be quickly discussing how and when to approach and restrain the patient.
4) Have strength in numbers. You MUST have enough people to manage restraining even a mildly agitated patient. Having at least one person for each limb, and one to distract the patient, and one to help with the restraints means having at least six rescuers involved.
5) Restrain supine. While there are several adaptations of this position, many experts are stating that this is the safest position for the patient. Use spit hoods if necessary, but make sure the patient is able to breathe easily and you can monitor their airway and level of consciousness.
6) Keep the patient restrained. Once the fight is over, patients may often ask to have a restraint loosened or released. As much as you might want to, don't. Remember, it may have taken six people to restrain the patient. Now, you are alone in the back. What are the odds of injury to you if the patient acts out again?
7) Above all, keep cool. The person tied down on the cot is a patient. Don't take things he or she says or does personally. Don't neglect your duties just because you might be angry.
=================================================================
What about using Patient Restraints?DEFINITION OF RESTRAINTS
Physical Restraints: are any manual method or physical or mechanical device, material, or equipment attached or adjacent to the patient’s body that the individual cannot remove easily which restricts freedom of movement or normal access to one’s body. Examples include, but are not limited to, leg restraints, arm restraints, vest or jacket restraints, waist belts, geri-chairs, hand mitts, wheelchair safety bars, and lap pillows. Center practices which meet the definition of a restraint include tucking in a sheet so tightly that a patient cannot move, bedrails, or chairs that prevent a patient from rising, or placing a wheelchair bound patient so close to a wall that the wall prevents the patient from rising.
Chemical Restraints: Psychoactive drugs used to treat behavioral symptoms in place of good care, such as using them for discipline or staff convenience.
WHY USE RESTRAINTS?
Physical Restraints: If a restraint is used to enable the patient to attain or maintain their highest practicable level of functioning then restraint use is justified. Some examples would include a half bed rail used by a partially paralyzed person to allow themselves to turn over in bed or a seat belt used to help remind double amputees that they cannot walk on missing legs (they may have the feeling that their legs are still there).
Chemical Restraints: Psychoactive medication may be given to treat a psychological condition, such as depression, that cannot be alleviated with restraint alternatives. Alternatives tried might include increased participation in activities, increased family visits and support, or 1:1 counseling with a social worker.
RISKS ASSOCIATED WITH RESTRAINT USE
Use of restraints can lead to possible negative outcomes such as decreased range of motion of the joints, decreased muscle tone, decreased ability to walk, lessened social contact, agitation, symptoms of depression or social withdrawal, incontinence and skin breakdown.
ALTERNATIVES TO RESTRAINT USE
1. Restorative nursing programs, such as walking, eating, toileting, bathing.
2. Correct wheelchairs that are in good working order and correct size for patient use.
3. Involvement in center activity programs to occupy patient’s time and attention.
4. Taped messages from family members to play when patient is agitated.
5. Toileting schedules for patients at risk to fall.
6. Using staff interventions and education to prevent triggering inappropriate behavioral responses from patients.
7. Use of safety devices that trigger an alarm when a wandering patient tries to leave a safe protected environment.
8. Use of body alarms that attach to chair or bed and alarm when patient tries to get up unassisted.
9. Use of a low bed.
The list of alternatives is endless. The key is to evaluate the patient and determine what plan of action can be put into place as an alternative to the use of a restraint.
This is only a guide and individual state laws must be applied if contrary to this guide. Restraining is one of the most sensitive and challenging aspects of nursing.
Restraints are often applied incorrectly and can cause injury and even death.
CHEMICAL RESTRAINTS:
They cannot be removed in an emergency.With belts etc., they should be quick and easy to remove in an emergency without undoing knots.Some emergencies are flooding, fire, chemical fumes, patient having a fit, even toiletting!Chemicals can cause mental and physical damage to the patient.
POLICY ON RESTRAINTS:
All facilities at one time or another will be required to provide a policy on restraints. When using them if they are needed, every organization should have a policy on the correct selection of restraints, fitting them and the use of restraining equipment. The Hospitals and Nursing Homes may appoint a qualified agent to assure that patients when needed are correctly and safely restrained, with the correct restraint for the patient’s and its current condition. If restraints are incorrectly fitted or the wrong restraint is used, they should educate the person who fitted it.
Most Hospitals and Nursing Homes do not like to restrain – so the less they restrain, the less familiar Patient Safety Officer and a committee to regularly inspect any restrained
restraints available and they should be consulted when selecting a restraint.
They should also inspect the restraints daily when fitted. It is important that there are Carers in every organization who have a good knowledge of the different restraints.
Staff should be given regular WORKSHOPS ON RESTRAINING and the alternatives to restraining.
INCORRECTLY FITTED RESTRAINTS MAY WORK, BUT…will not be able to stand up. However, may slide down and strangle themselves. Remember that normally chair restraints are wrapped once around the rear legs of the chair at the pelvic position, before buckling together. There are many ways to put a belt on incorrectly, and they may still work.
FURTHER INFORMATION:
The qualified care-giver and the reaction from the patient, see how the patient accepts the restraint. Never apply and neglect a patient. Always see how a patient reacts when restrained for the first time. Do some ‘trial runs’ restraining the patient, soon as the patient starts to resist the restraint, the Care-giver may need to remove it and find out why the patient is restless.
In the case where the need for the patient to be: toilet; hungry; thirsty; TV is too loud/soft; wrong station; – does not like the face opposite them, etc., consideration for an active restraint should be considered with authorization from qualified facility supervisor.
The patient can sit for a long time and not need a belt. Care-givers should never neglect the patient, so as to try to find out what upsets the patient and correct the problem. If they can walk, try to walk and exercise the patient.
Dementia patients may play with the buckle, alter the size, then slide down and strangle
themselves. For hyperactive patients, the ‘Chair Belt for Sliders’ is very safe, and allows movement without being too restrictive. This is safer than a ‘VEST’ type of restraint.
FOR DEMENTIA PATIENTS:
Do not use Lap Belts that can be made bigger without undoing the recommendations, ask them to sign a form to decline restraining, despite the Care-givers assessment of
the risk for the patient or other patients or staff. If the patient’s relations or doctors do not want to restrain the patient, and the qualified facility supervisor insists on over-riding the Care-givers request for fixed restraints, contact your supervisor and made sure you chart the incident and request for pending or non-pending patient restraints.
Restraints are designed to take into account safety, dignity, incontinence, ease of application. Instructions and labels with drawings are fixed on the restraints to assist the care-giver in support of correct placement onto the patient.
Patient Restraints and Other Alternatives
What Family Members and Friends Need to Know
Caring for someone who is confused or combative can be hard to do. These patients can fall and injure themselves. They can wander to unknown areas and get lost. Combative patients can strike out and injure staff or family members without meaning to.
While no one wants to see someone in danger of harm, the solutions are not simple. Years ago, nurses and doctors quickly placed confused and combative patients in restraints. They did this to assure safety. Today, in our hospital, restraints are only used after other options have been tried without success.
Adopting “Restraint-Free” Approaches
Today, with the support of a federal mandate, nurses and doctors try many other options before placing restraints. Many hospitals and nursing homes are adopting a restraint-free approach. This promotes safety and allows the patient to be mobile. Ways that can help to keep a patient restraint-free are:bring in objects that are well-known to the patientkeep the patient’s daily routine and rituals that they are used to help the patient maintain his or her ability to walk (when we are able to do this)keep a watchful eye on the patient when restraints are not in use
As much as we try, we are not always able to keep patients restraint-free. At times, restraints are the best choice. The rest of this handout helps to answer common questions that people often have about the use of restraints. Please read the entire handout. If you have any concerns, talk with your doctor or nurse.
What are Restraints?
Restraints are devices used to restrict freedom of movement. Their purpose is to prevent injury to the patient or others. The most common types of restraints are belts and soft wrist restraints. These are used to tie a patient to a bed or chair. An enclosure bed may also be used. This is a box shaped tent-like structure that fits over the patient’s bed. The sides are made of mesh and can be zipped open and closed by the nurse. It provides a safe space in which the patient can freely move around in her bed. This is used mainly for patients with impulsive behavior. It may also be used for patients with seizures who are at risk for falls.
Why Use Restraints?
Restraints limit movement and prevent injury. They can be helpful to nurses and doctors as they provide care. Restraints can also be used to:keep the patient safe and prevent fallsprevent injury to family members and staffprevent patients from pulling out tubes or taking off dressings
According to the 1992 federal guidelines, if patients have life-threatening symptoms, restraints may be used short-term to help with lifesaving treatments. They may also be used if the patient’s behavior is posing a threat to the safety of others.
How Long Does a Patient Need Restraints?
The amount of time restraints are used depends on how well the patient is oriented and able to follow simple commands. As the patient gets less confused, the staff will try many times a day to remove the restraints. When they are off, family members or staff might need to be present. The staff will teach you how you can be most supportive during those times.
Who Decides to Place Restraints?
Restraints are used as a last resort. The decision to restrain a patient is made by one or more members of the patient’s treatment team. This includes doctors and nurses. If the patient cannot partake in the decision, a family member is consulted if possible.
How Can I Be Assured that Someone is Safe While in Restraints?
Nurses and others will often check the patient’s safety and comfort. At least every two hours, the restraints will be taken off for daily activities. This may include eating, going to the bathroom, and exercise. The hospital has policies on caring for patients in restraints. Staff are trained to be sure all patients in restraints are closely checked.
What Measures Do We Take to Assure the Best Care?
When restraints are used, it’s important to let people know why they are being used. Patients will sometimes fight against restraints and want them taken off. This is when it’s useful to talk with the patient about what they can do to have the restraints removed. Your nurse will talk with you about specific behaviors the patient needs to do in order to get out. For example, they must follow simple commands and leave tubes, IVs, and other devices in place. This helps us to know that the patient is less confused and is thinking more clearly.
What Does It Feel Like to Be Restrained?
This can vary. Some patients are not aware of the restraints. Other patients might feel lonely or isolated. Still others feel angry, fearful, or humiliated. You may hear your loved one ask, “What did I do wrong?” They might feel like they are being punished.
How Can I Support the Patient While Restraints Are in Use?When you can, it is best to stop by the nurse’s station before you enter the patient’s room for the first time. This will give the nurse a chance to briefly tell you about restraints and why they are being used. This is a good time to ask questions.
Often restraints are used because someone is confused. Therefore, it’s best to try to do things that help the patient get reoriented and less confused. It is helpful to tell them: who you arewhat day it is where they arewhy they are restrained
Asking questions that require brief or one-word responses helps a patient to feel more in control. Simple, short answers to questions also help a patient to understand your response.
Placing calendars and clocks within sight can help to keep the patient oriented to date and time. Reading current magazines or news articles to a patient helps to keep them oriented and current.
Short frequent visits are best. Having someone come in and out of the room gives the person a sense of support and safety. It helps to conserve the patient’s energy while providing reassurance.
You also need to be aware of your safety and the safety of the patient. For instance, giving a glass of water rather than a hot drink can prevent spills and burns. Using paper or plastic dishes and utensils are safer than glass ones. Cigarettes and matches should never be given to a confused patient. And certainly, no medicines or sharp objects that could be harmful should be left within reach.
Patient restraints :
The use of restraints can be stressful for patients and their families. We created this handout to answer some of your questions on the use of restraints.
Sometimes illness, injury, medications or being away from home can cause a patient's behavior to change.
At Hamilton Health Sciences we have a policy of Least Restraint and we try very hard not to use restraints where possible. When used, they are a temporary measure to protect the patient's health and safety and that of others.
What are restraints?
A restraint is a method used by the staff to restrict movement by the patient.
What are other options to using restraints?
There may or may not be other options. When there are other options, we will try them first. We encourage family and friends to help us understand the patient's needs and choose suitable options.
Some other options include:
• sitting with a patient
• walking with a patient to get rid of pent up energy
• playing a patient's favorite music at the bedside to calm him or her
• having regular supervised toileting times to assist unsteady patients
We may ask family or friends to help with these options.
What are the types of restraints used?
There are different types of restraints: Physical restraints
• worn by a patient to restrict movement
Chemical restraints
• medications used to control aggressive or agitated behavior
Confinement or Environmental restraints
• a change in the environment which restricts movement from one area to another
Monitoring devices
• a device used to monitor the patient’s movement